Really sorry to hear this, it is a total mess because decisions are being made quickly based on very broad categories and I suspect there is a lot of interlinking of policy-making that we don’t understand. And I hate to say it, but I suspect financial considerations will be in the mix in terms of decision making as well. I imagine that to support all the people in the ‘vulnerable’ group - with the very many conditions policy makers decided to include within it without any recognition of the massive variation of experience of people within each category- is not financially viable and therefore we are left with vague and unclear advice much of which many cannot follow due to exactly the type of situation you find yourself in.
I think big questions remain unanswered and this leaves people vulnerable for a number of reasons. I’m still unclear on some pretty big issues:
What is the degree of risk of complications faced by people with Parkinson’s who have no history of breathing difficulties?
While this potential complication of the condition is an extremely serious concern for those experience it, breathing difficulty is not listed as a key/ defining feature of Parkinson’s in any of the NHS or PUK’s literature. I’ve looked around but am struggling to find any statistics as to the demographic of the Parkinson’s population who experience this complication at any specific time or, in fact, any advice or information sheet on this symptom that we are now all being defined by. I am no medical expert so it’s not that I’m disagreeing, I just don’t understand what I am being told. Is there any information in relation to this subject?
Why are we suddenly losing our right to be viewed as individuals?
What’s happened to ‘Understanding Parkinson’s’ and the wide range of symptoms, ages, general health and stages of condition that means that each one of us is having our own experience of this condition at any given time?
How are people supposed to implement the advice given when they have no financial protection or other support in order to do so?
What is the point in central government labelling huge amounts of people as ‘vulnerable’ and then giving them no practical help to implement the advice being handed out?
In fact, what exactly is the point/purpose of the ‘vulnerable’, but not ‘very high risk’, category?
What would actually make sense was if decisions were made on a case-by-case basis by GPS and medical practitioners who actually know what they’re talking about but I suspect this would be considered too expensive and unmanageable.
I currently have no breathing issues in relationship to Parkinson’s Disease and although I do have some challenges, I live independently and exercise quite a lot. I don’t feel that I should be on the ‘vulnerable’ list because while I am, I feel that I have to follow advice as best as I can which means that I am shamefully scrambling for online shopping slots while I know that people in much greater need can then not have one - and the irony is that I am more capable of getting a slot than many people who are in need because I am in much better health. I’m not, however, totally sure of the implications or consequences of not following advice because there is so much that I don’t understand about decisions being made.
The guidelines that exist are somewhat meaningless for many, many people in the ‘vulnerable’ but not ‘at high risk’ group. I’ve said this already but I don’t understand the reason for this categorisation if it has no practical impact on people’s ability to look after themselves. The contradictory and unclear information out there is leaving people in complete limbo and I very much feel for you and the position that you are in Jx
GP has recorded on my gp records that im advised to stay home snd not goto work so i can print it off and send to boss . So i am being furloughed so get 80% of salary
V relieved
Jackson expressed fear about treatment options for coronavirus being affected by having the underlying illness of PD. Medical ethics would actually prevent that, but the BMA has now issued specific guidance on ethics, which makes that clear.
Hi Jane, thank you for posting this - it’s interesting. I really just want to understand the position I’m in in relation to everything that I’m reading in order to get some sense of control over things but it’s really hard to find any clear, open and consistent information. I’ve been reading the official guidance on the NICE website, though I’m trying to reduce looking up information so that I don’t drive myself dotty. Although I’m not in isolation, I might as well be because I live on my own in a city. Driving to a rural area to ‘get out’ is not permitted and you’re not allowed to meet up with people you don’t live with. I do understand the reasons for these measures but it is still tantamount to enforced solitary isolation. I have way too much time on my own with my ‘Parkinson’s brain’ and I’m already fed up with social media. I like researching things but I tend bug people and/or find answers that I don’t like so maybe I need to stop :-s Thanks again. Hope you’re still doing ok. Jx
For myself, I have made the decision that if I get the virus and need hospital treatment to survive, I will refuse it and just ask them to make me comfortable at home. There are a number of reasons for this, but the main one is that with the delights of end-stage PD to look forward to, I think a healthy, younger individual needs a ventilator more than me.
Hi Jane,
Thank you for sharing your thoughts. It’s a tricky conversation to have but I think by shying away from such issues, we give them more power to exert fear over life in the here and now. It’s just a personal viewpoint but in the current situation, I think discussions about end of life care need to be held openly; I am not willing to live whatever life I have left hiding in fear of both an unseen virus and a system that I don’t understand so I need to gain understanding so that I can make decisions and exert a degree of control over my fears.
We both know that everybody will have a different opinion about this depending on their individual belief set and situation and are not trying to impose our own beliefs on anybody - it is such a difficult thing to have to think about.
I would like to write my wishes down for any number of situations I may find myself in, and it may very well be that in certain circumstances, my choice would be the same as yours, but in order to do this I would like clear information so that I can base my decisions on whatever factual knowledge exists .
I’m also trying to gain understanding in case I am put in the awful position of needing to make, or contribute to, a decision on end of life care for somebody close to me.
It is incredibly difficult but more information is needed so that people understand the potential consequences of any decisions they make and at the moment, people are floundering.
Take care. Jx
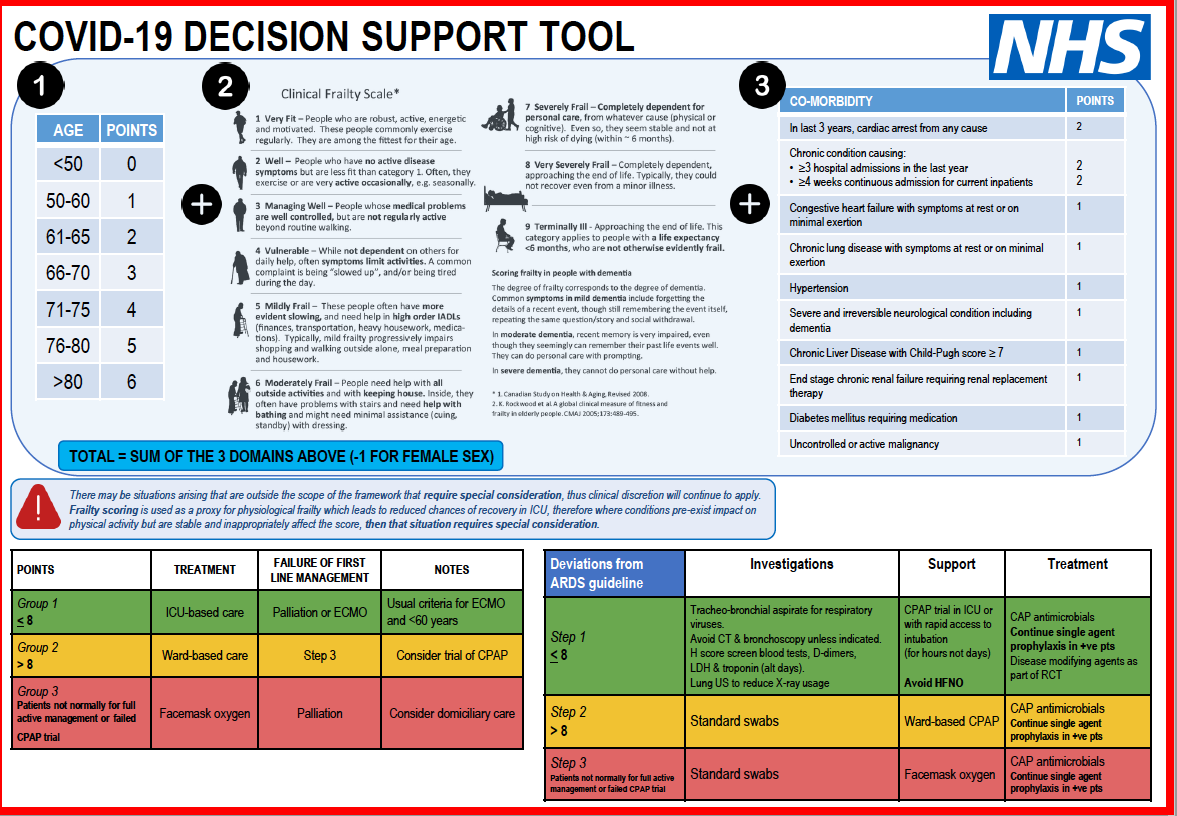
The Financial Times has published a document distributed by NICE to help doctors ‘score’ patients to decide which patients receive critical care. Unfortunately I don’t think I can link to it from this forum, because the FT has a paywall, so I will try to describe it.
The scoring is in 3 parts. The first is age: under 50 no points, 50-60 1 point, 61-65 2 points, 66-70 3 points, 71-75 4 points, 76-80 5 points, >80 6 points.
The second part is a clinical frailty scale, which in nine levels from Very Fit to Terminally Ill.
The clinical frailty scale is complicated for people with PD because our individual capacity can vary so much from day to day or even hour to hour. I could place myself on it anywhere from stage 3 - Managing Well, to stage 6 - Moderately Frail. My tip: if you want to maximise your chances of getting a ventilator, insist you are capable of cooking and heavy housework!
The third part is points given for Co-Morbidity, which seems to mean existing serious and chronic conditions: I won’t type the whole list, but a heart attack in the last three years is 2 points. PD scores one point, as does diabetes.
Then a point is taken off for being female.
I get 3 points for age, between 3 and 5 points for clinical frailty and 1 point for co-morbidity. Then I lose a point for being a woman, so my total is somewhere between 6 and 8. If I were anxious to survive, that would be reassuring, since 8 or less points qualifies for ICU based care.
Hi Jane,
I saw this too. It’s a document that is not on the NICE or NHS websites as far as I can tell so it’s hard to know where the Financial Times got it from unless I missed something - though that is always very possible :-/ It looks like a PowerPoint slide so it may be a discussion document as opposed to to something that is actually in usage but I still think it is very concerning.
My parents would be devastated to see this and so would many other people. In fact I know of far too many people who are currently living in total fear of the ‘implied and the unknown’. I know of people who are sitting drinking themselves silly in an attempt to get through this and I know of people who are very frail and yet are still sitting up all night panicking as to where they are going to get their weekly shopping from.
The advice to take exercise and eat healthily and keep yourself sane is very hard when you can’t actually get any food or toiletries.
This situation is not going to be over anytime soon and I don’t think it’s in any way acceptable to keep vulnerable and elderly people existing in such a state of fear and isolation in the name of ‘keeping them safe’. I continue to feel very strongly that politicians and decision makers need to be honest with the general population about the reality of the situation - but then again I’ve been told that I can be horribly opinionated with an awful tendency to get on my high horse at the drop of a hat and I don’t think spending 24/7 alone is helping me to keep my less pleasing character traits in check:-S
I wrote to the Hepline about this a while ago and they were very lovely and passed me on to the Excellence Network. I’ve had an acknowledgement rather than a response but it’s a tricky question that I’m asking so I’m still hopeful of getting a response.
Hope this finds you well.
Jx
It isn’t clear to me what the alternatives are, or what you think should be changed. The triage procedure will have to be used if there are not enough ICU beds or ventilators for all who need them. The medics will have to make horrible choices, often very quickly, and guidelines that ease the process will be necessary.
It would have been better if our government had been funding the NHS more generously instead of running it on a shoestring, had prepared for pandemic, and taken action sooner after the WHO declared a global emergency. But they didn’t and so we are where we are.
Hi Jane,
According to the Daily Mail (view that as you will :-S) the scoring system was a proposal that is not being used. I’ve interpreted the article as saying that it was unreliable and crude, but that could just be me imposing my opinion.
In terms of alternatives, I don’t know. I am, however, confused by the somewhat tepid lockdown that seems to make our approach different to that across much of Europe. I’m not sure what our current Government’s ‘endgame’ is and I’m not totally convinced that they have fully ditched the original ‘herd immunity’ strategy, but who can tell?
Of course nobody has the answers but I’m just not willing to quietly ‘take one for the team’ and accept my status as disposable without at least understanding the basis, ethics and evidence for such a decision being made.
My main point is that there has been, and still is, no engagement with the general public about this issue and there seems to be no appetite for the honest and open discussions that are both good practice and necessary; but there needs to be a discussion because we all need to work together to get out of this and we can’t do that if we don’t understand what we’re working on.
I’ll do what is right for me within the constraints of the situation I find myself should I get this virus but I’m going to do it noisily because the policymakers need to understand the position that they have been at least partially responsible for getting us in to so that when this all finishes, and it will, the sacrifices made do not just get brushed aside; and they will do if there is no public acknowledgment of the policies that are being put into place in the first place.
If I am to be told that my life is not worth as much as somebody else’s because I have Parkinson’s Disease, then the least I would like is to be informed of this honestly and openly and be allowed to ask questions about this decision. If the situation then arises whereby I might need hospital care, I will fully understands all of my options and can make choices accordingly.
This is just my opinion. We are all different. None of us ever imagined we would end up in this position and we all have to work our way through it as best as we can but some honest and open leadership ( in fact any leadership :-S) at all levels would help. x
 Jx
Jx